The potential implications of government COVID-19 publications for adults with a learning disability and specialist learning disability services
Dear colleagues
I hope you are keeping well. These are very concerning times for us all professionally and personally. I am certainly worried about the impact this pandemic will have on adults with a learning disability both during and in the aftermath of the situation. Therefore, in my role of Research and CPD Officer I thought I would share some of the recent publications coming from the government about COVID-19 and the potential impact they could have on adults with a learning disability and learning disability services both in the short and long term. I am also sharing some snippets of what we are doing locally to try support adults with a learning disability and their network of care. Of course, the response of your services to the pandemic will differ depending on the local population, drivers, services and the severity of COVID-19 in the area.
The first government publication to be released that directly related to adults with a learning disability was published last Tuesday the 17th March. Guidance on social distancing for everyone in the UK stated for the first time since the pandemic that adults with a learning disability would be seen as a high risk group for developing severe illness from coronavirus (COVID-19). Therefore, the government recommended that they should be particularly stringent in following social distancing measures. This advice seems such a long time ago now we are all on the same restrictions with social distancing, but at the time it helped to give some clarification to what we already knew.
Locally, the publication meant we could officially suspend all non-essential physiotherapy services for adults with a learning disability to reduce the risk of them contracting COVID-19. I am sure you were all anticipating this happening, we certainly were, so it was helpful to have it documented. In response, we developed a database of adults with a learning disability that had a physiotherapy need and we viewed at high risk of severe illness from COVID-19 and have been proactively contacting them to discuss the pandemic and social distancing. Offering support where possible to try to reduce their need to access primary and in particular secondary healthcare. We have developed MDT plans to actively monitor this group of people throughout the pandemic.
Since this first publication on social distancing, the preparation for the impact COVID-19 is going to have on health and social care has been ramped up significantly. Much of the guidance has been targeted at acute services and getting them ready for the influx of patients. Until the government released “COVID-19 Hospital Discharge Service Requirements” on the 19th March 2020. The document outlines where allied health care professionals are likely to be needed to support the COVID-19 pandemic. It essentially outlines how the government propose to discharge anyone who is clinically safe within 1 hour to free up beds.
The government anticipated that 50% of patients will need a simple discharge with no follow up for health or social care; 45% will require support to recover at home; 4% will need rehabilitation in a bed based setting; and 1% will need to stay in hospital. Clearly, this strategy means a lot of people will be discharged home who require follow up in the community through a Supported discharge/Rapid Response service. The paper states that:
A lead professional or multidisciplinary team, as is suitable for the level of care needs, will visit patients at home on the day of discharge or the day after to arrange what support is needed in the home environment and rapidly arrange for that to be put in place. If care support is needed on the day of discharge from hospital, this will have been arranged prior to the patient leaving the hospital site, by a care coordinator
The onus is making people safe on discharge rather than on rehab which could have significant implications for long term disability and recovery from acute events and conditions such as neurological events, falls and fractures.
Although this paper does not directly discuss adults with a learning disability or specialist learning disability services, the government does state that community team must:
Release staff from their current roles to co-ordinate and manage the discharge arrangements for all patients from community and acute bedded units.
There are a number areas outlined within the document that specialist learning disability physiotherapist have the skills to be redeployed. Therefore this could significantly impact on the delivery of services to adults with a learning disability during the pandemic and after as services recover from its impact. The NHS is proposing to pay for the implementation of the document and it will completely change service delivery for the duration of the pandemic. It is likely to take years to recover from the situation, if ever. And this could impact of specialist learning disability services, especially those smaller teams where the entire MDT is absorbed into supporting the situation.
Locally we are working hard to ensure that we maintain a role in supporting adults with a learning disability and their network of care during this period by preventing their need to access primary and secondary healthcare and supporting our social service colleagues. We hope this will also safeguard services for adults with a learning disability once the situation resolves.
The document also has a direct impact on adults with a learning disability in hospital during the pandemic who may not be able to return home. The government state that:
During the COVID-19 pandemic, patients will not be able to wait in hospital until their first choice of care home has a vacancy. This will mean a short spell in an alternative care home and the care coordinators will follow up to ensure patients are able to move as soon as possible to their long term care home.
This means adults with a learning disability could move to mainstream nursing homes wherever there is a vacancy.
Finally, and possibly most concerning, was NICE COVID-19 rapid guideline on making decisions for critical care treatment during the COVID-19 outbreak.
https://www.nice.org.uk/guidance/ng159
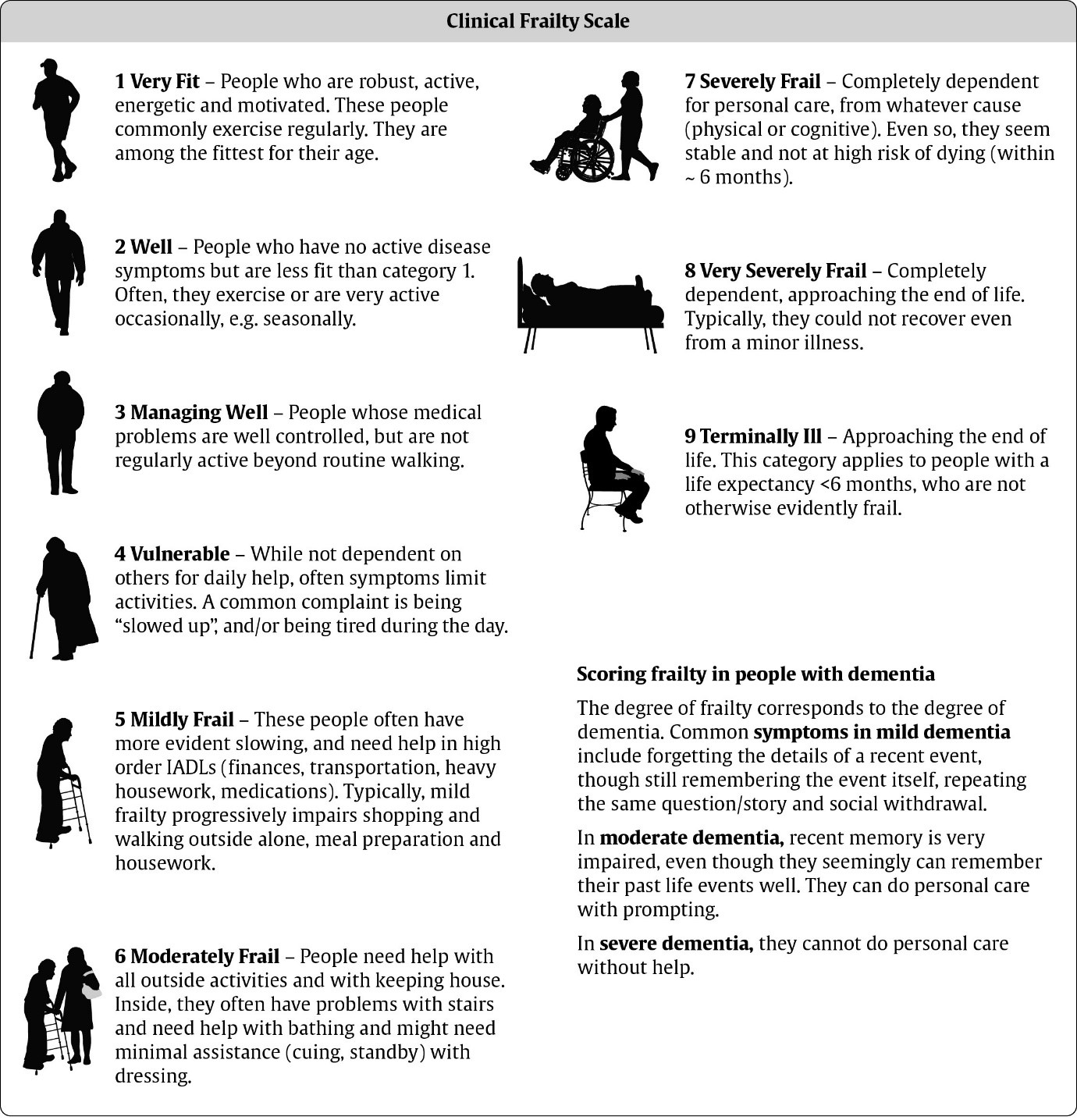
This document recommends using the Clinical Frailty Score, co-morbidities, preferences, wishes, and predicted clinical outcome to indicate when someone would be eligible for a critical care bed during the high demand caused by COVID-19. The use of the clinical frailty score as an indicator significantly impacts adults with a learning disability, especially those with an associated physical disability. Chris Hatton, Professor of Public Health and Disability at Lancashire University wrote a blog outlining these concerns (https://chrishatton.blogspot.com/). This is worth a read, he outlines the concerns more articulately than I could.
Since the publication, NICE Coms have published a statement via twitter acknowledging that the clinical frailty score should not be used in adults with a learning disability or people with cerebral palsy.
@NICEComms posted at 19:42 on the 23rd March 2020
NICE is very aware of the concerns of some patient groups about access to critical care, and we understand how difficult this feels. (1/5) Our new COVID-19 rapid guideline on critical care was developed to support critical care teams in their management of patients during this very difficult period of intense pressure. (2/5) The guideline says that on admission to hospital, all adults should be assessed for frailty, and that other comorbidities and underlying health conditions are also taken into account. (3/5) The Frailty scoring system is not perfect, therefore we recommend that Clinicians should take any decisions about care in conjunction with patients and their carers where possible. (4/5) We welcome the recent clarification that the Clinical Frailty Score should not be used in certain groups, including those with learning disability and cerebral palsy, which we will reflect in an updated version of our guideline. (5/5)
NICE updated the guidance in the 25th March 2020 to clarify that the Clinical Frailty Scale should be used as part of a holistic assessment, but should not be used for younger people, people with stable long-term disabilities, learning disabilities or autism. NICE now recommend:
On admission to hospital, assess all adults for frailty, irrespective of COVID‑19 status.
Use the Clinical Frailty Scale (CFS), available from the NHS Specialised Clinical Frailty Network, as part of a holistic assessment.
Be aware of the limitations of using the CFS as the sole assessment of frailty. The CFS should not be used in younger people, people with stable long-term disabilities (for example, cerebral palsy), learning disabilities or autism. An individualised assessment is recommended in all cases where the CFS is not appropriate.
Consider comorbidities and underlying health conditions in all cases.
Record the frailty assessment in the patient's medical record.
[amended 25 March 2020]
{kind=link}

NICE now recommend that clinicians complete an individualised assessment in all cases where the CFS is not appropriate. Specialist learning disability physiotherapists have a key role to play in supporting the individualised assessment of frailty and potential best interest decisions whether the person would be eligible for a critical care bed. For this reason, we should be actively monitoring adults with a learning disability locally during the COVID-19 pandemic with the aim to reduce risk of hospital admissions and be proactive in identifying if someone is admitted to hospital. I am aware the NICE guidance does not cover Scotland.
I hope you have all found this a helpful summary. By the time you have read this everything could have changed! Adults with a learning disability and their network of care need our support more than ever.
I know you are all incredibly busy, but if you can spare some time please share how you are preparing for the pandemic locally it would be really helpful. We are all in a quandary about how we can best support our service users during this difficult time so learning from others is key.
If you email these to me I will collate them and then send them and upload them to the website.
David Standley, Research and CPD Officer. david.standley@gstt.nhs.uk
Number of subscribers: 9